In November of 2017, it was recommend start to integrate deadlifts into my strength training regime. Under the supervision of an experienced body builder, I did around 20 deadlifts with what I thought was a “okay” amount of weight. The tiny gym I was at did NOT have a hex bar as shown above. Later than night, but lower back was killing me. The pain eventually went away so about a 10 days later I attempted a few more with almost no weight on the bar itself, yet afterwards I was in pain again.
In early 2018, I had a major bout of sciatica, presumably caused by dead lifting, where nary a chiropractor, massage therapist or physical therapist could fix it. I finally went to my family physician and he prescribed Pretoszone. Within 48 hours the pain was gone. The P.T. said he never recommends deadlifts for strength training.
Fast forward three years: for the past nine months I have had what feels like a pinched nerve causing premature pain or weakness in my right leg while cycling more than 60-90 minutes (sometimes while backcountry skiing & usually while hiking). This is despite a professional bike fit with a P.T. with a pressure mapping saddle system. The pain is always on my right leg, which is where my sciatica left off. Ibuprofen will remedy the situation, but I don’t want to have to take that before every single ride! Preliminary diagnosis is that I have EIAE (External External Iliac Artery Endofibrosis), but further testing or imaging is needed. The vascular surgeon I met with in 2019 recommended I hang up cycling and find another sport that doesn’t pinch my artery while cycling, but the problem also persists with other sports.
Long story short: deadlifts are dangerous, especially for tall people like me (6′ 3″). If you feel you MUST do them, I highly recommend a hex bar. Below are some of notes about deadlifting for tall people.
Do leg press instead of Squats. 80% as good with 10% of the risk. Never use a leg press if you have existing back pain and always consult a physician first if you are over 45. Finally, movements that put direct downward pressure on the spine, such as squats and dead lifts, are proved to be effective in preventing osteoporosis. https://www.fitness.com/articles/1013/squats_and_deadlifts_after_40_don_t_do_it.php
If you’re new to deadlifts or have questionable form I’d start with high handle trap bar deads. Stick with these for at least six months and never go above five reps. But if for some reason you can’t deadlift, it’s nothing to get down about. You’ll be just fine with squats, Olympic pulls, shrugs, glute hams and the like. http://jasonferruggia.com/drop-the-deadlift/
Don’t bend knee more than 45-degrees. The most common mistakes, says Woll, are allowing your head to pop off the bench, with your chin tucked, or allowing your lower back to do the same. “We all have lower back issues, so we never want to ‘load’ a lower back,” Then remember that the back of your head and from the middle of your spine all the way down to your hips should be flush against the bench, she says. https://www.huffingtonpost.com/2012/08/28/fix-your-form-how-to-exercise-leg-press_n_1833521.html
eoGEAR Fuel Box holds mixed nuts or six fig newtons perfectly.
Despite that I sell “tech” bike food on my site, I frequently get tired of it on long rides (300K +). I consequently designed a top tube bag that enables me to have food conveniently in front of me, w/o the need of reaching back to my jersey pocket (which is frequently covered with a jacket during all night brevets anyway). I also have a “mini food box” insert, which I place inside this bag for real food.
My new favorite cycling food, which sustained me through my last ”straight through” 600K, is steamed red potatoes. I add a salt and pepper and quarter them with the skins left on. I also supplement this with Perpeteum or Accerlade as the potatoes provide lots of carbs, but little or no protein. I also like PB&Js a lot, but they dry out quickly when I have them in my top tube bag so I sometimes put peanut butter inside a rolled up flour tortilla. Fig newtons are also one of one of favorites. A recent article in Bicycling Magazine endorsed these as the best pick for convenience store choices.
I think my favorite “provided” food is the soon-to-be world-famous tortilla wraps provided by Susan Plonsky (RUSA RBA, Ariz. ~ 2012). Those are worth the 10-hour drive to Arizona! (Ham and/or turkey, cheese and a little potato salad in them along with other secret ingredients that she is always changing so I can’t copy the recipe).
As far as tech foods go, I like Cliff Bloks (carbs only) and also the new Clif Roks, which are laced with some protein. I usually have two “water” bottles on my bike, one with water with an electrolyte additive (Elete brand in liquid form) and the other with a flavored sport drink like Perpeteum (also adding Elete to it, as oddly enough, Perp. has little or no electrolytes) or Cytomax sports drink (no need to add Elete).
I have a weakness for pastries, so at convenience stores, I usually go for a donut, muffin, sweet roll or a packaged danish, but I have heard that after three hours of endurance activity, one needs to start ingesting more protein, not just carbs. Sometimes I get a small sub sandwich with lean protein, like ham or turkey, in an effort to get some protein into my system. I also do mixed nuts combined with other small things like Peanut M&Ms. I always bring my own Heed or Accerlade powdered mix, pre-measured in small Zip-Loc bags and mix with the water from the c-store fountain.
> Richard (this is a copy of an e-mail I posted on a Randonneuring forum, Feb. 2011)
My first long ride on a road bike was a typical 100-mile charity “century” ride. That is where I first come to realize that neck pain was commonplace for many roadies. Since then, I have ridden thousands of miles, mostly using bicycles with aerobars. I use the aerobars for two reasons (#1 is the most important): 1) As a 6′ 4″ tall person, aerodynamics on a road bike has always been an issue, so I adopted the use of these to limit my wind resistance. 2) Changing out of hand positions. Using aerobars enables me to move around more on the bike to limit the pain in my hands and lessen the fatigue in the upper body.
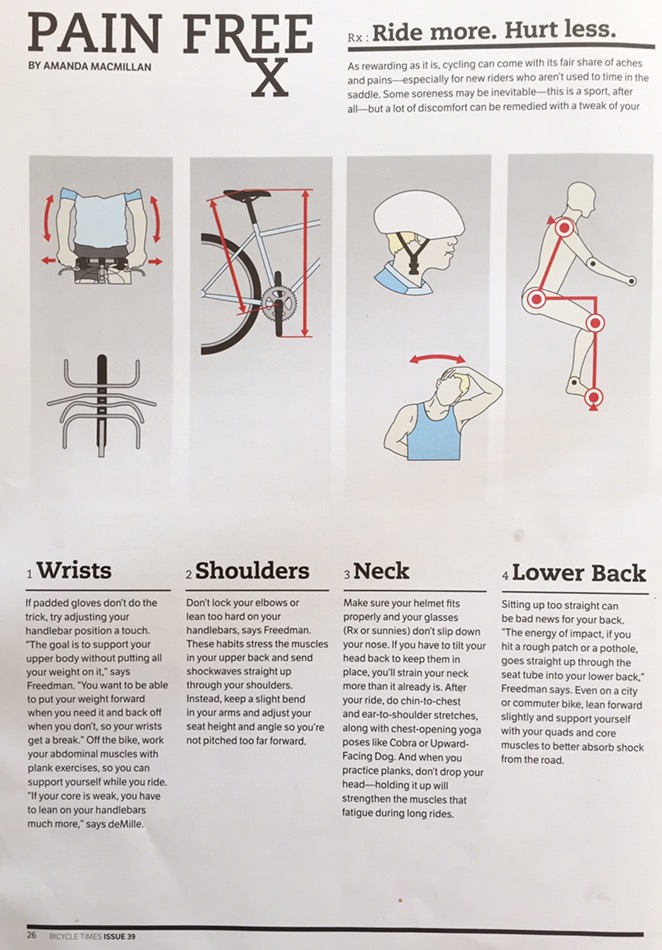
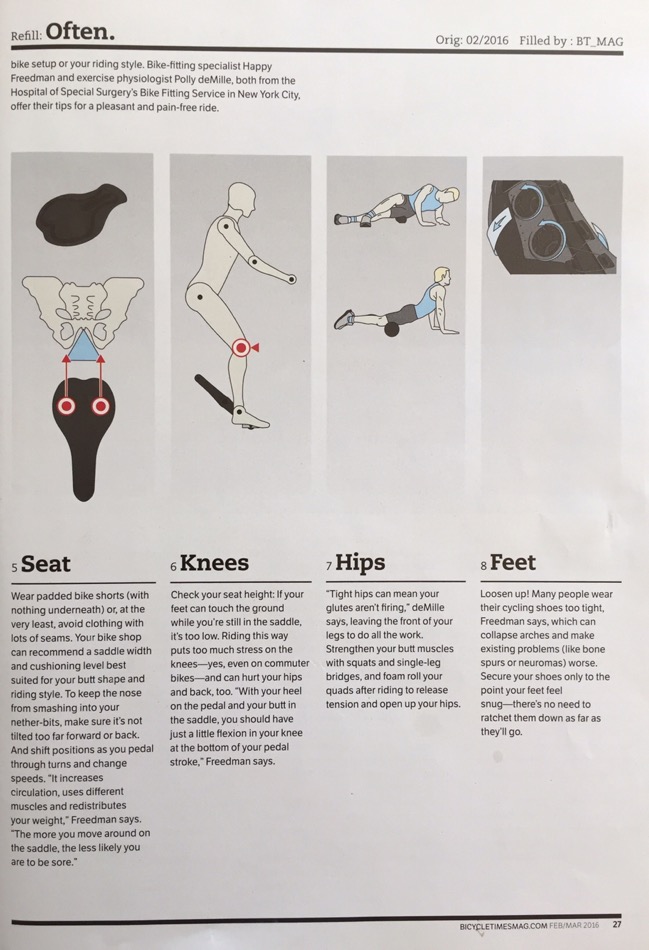
Recently I saw this article in the March 2016 issues of Bicycle Times magazine and have reposted it here (used by permission). Points two through four are relevant to neck pain.
I have consulted with my nephew, Jeremiah DeLlamas, who is a seasoned physical therapist. Below are his suggestions on how to alleviate soreness when riding.
When I ride, I really try to consciously remind myself to perform chin tucks and shoulder retraction exercises or Shoulder pinches. Because of the rounded shoulders and forward head in the extended position, this puts a lot of stress on the posterior disc of the cervical spine and deep cervical musculature. Try to deep the chin tuck exercises and this will help activate the deep cervical muscles as you are riding. Every 20-30 minutes remind yourself to do 10-15 chin tucks holding for 5 seconds. Stop in at the building when you are in town and we can go over more.
My takeaway from his suggestions was to regularly tilt my head down (aka chin tucks) while riding. I used to only turn side to side, which providing marginal, if any, benefit.
Hopefully, these suggestions will allow you to go further and/or faster, while minimizing your pain threshold!
Several large manufactures have lately been putting more emphasis on visibility, not just comfort and speed while cycling. This is especially notable with the numerous distracted drivers these days. They include Trek and Pearl Izumi.
Also see this article published on the RBR website. (It clearly states that blinking tail lights are better than solid…something I have always agreed with).
Apparel
In a brochure published by Trek, they suggest three basic ABC rules. “A” means always-on lights; “B” means biomotion, i.e. careful placement of materials and “C” means contrast to aid in visibility. Having brighter colors on ones feet and/or ankles is perhaps more important than having a visible jersey, because those parts are moving while you cycle (Pearl Izumi also calls this biomotion).
For night riding, I have always worn reflective ankle bands, but had not considering wearing bright socks, which serve a similar purpose. Consequently, in the spring of 2017 I purchased several pair of the flo-green DeFeet cycling socks (Aireator 5″ D-Logo Hi-Vis Yellow w/Hi-Vis Green – Double Layer Cuff).
“Fluorescents, like our iconic Screaming Yellow, actually convert invisible UV light into additional visible light. Typical colors reflect a maximum of 90% of light vs. 200-300% for a fluorescent color.”
They suggest that there are three key factors in getting driver’s attention:
True Fluorescent Colors
Biomotion
Contrast
I see so many roadies wear “cool and groovy” black jackets or jerseys. Dumb. For mountain biking it doesn’t matter, but for city road use..be smart!
Daylight Running Lights
Trek, in their brochure, is also emphasizing the importance of using daylight running lights, both front and rear. See this page for a video and additional info.
They mention three factors in lighting for cycling:
Focus
Flash
Range
I adopted daylight running lights several seasons ago, using some tiny, but powerful USB rechargeable lights by Leyzne. (See this page on my site for more info on tail lights).
Video Capture
A few cycling friends are now mounting to the rear of their road bikes, rear blinkie lights that also have a mini video camera built in. It runs an endless loop so you will have a record of any collisions or close calls. (See this video of a guy getting hit by a car, as shot by his friends GoPro helmet camera).
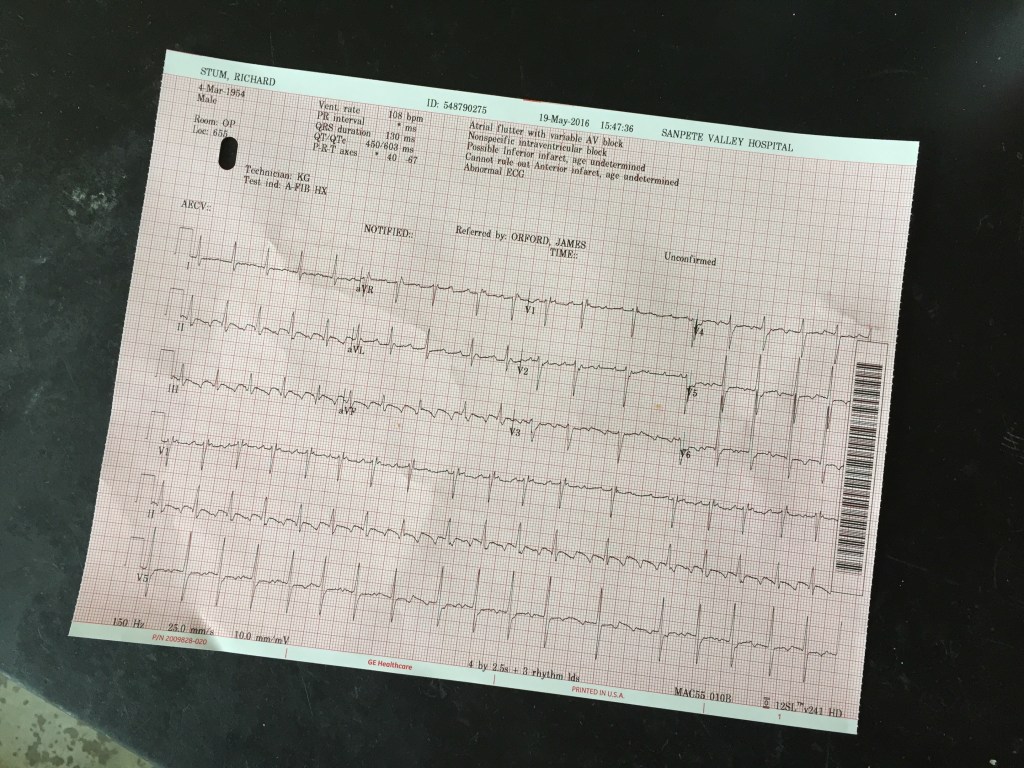
On February the 20th, 2016, I had a mild ischemic stroke — while resting at home for the weekend. A CAT Scan showed no damage in the brain, whereas the MRI showed many small specs, clear evidence of a stroke in the left frontal lobe. It was later determined that the cause may have been a PFO (small hole between the two heart chambers). This is called a cryptogenic stroke (unknown cause, which happens in 40% of stroke victims). As a ultra-endurance athlete with no history of heart disease or stroke, I was blind-sighted by this. I have no long-term affects from the stroke. Later, the cause of the stroke was found to be a giant Lambl’s excrescence, a benign tumor or lesion on the aortic valve of my heart. On May the 10th I had open-heart surgery to remove it. The surgery went fine, however because my sternum was cut down the middle, the physicians banned me from cycling for most of the summer, until it was completely healed, fearing that a crash on a bike would be catastrophic. Meanwhile, I needed to train for a Mount Rainer mountaineering “family” trip, which had been calendared from the prior year, so I started walking and eventually trail running. Normally, I have not had much luck with running, due to an old ankle injury, but with the aid of a new style of ankle brace, it was able to get back on my feet again (literally). I am now back on the path to “normal life” and hopefully many stroke-free years ahead.
The Full Story
Full Story Preface
Starting in Thanksgiving of 2015 and running through February of 2016, I was getting consistent (approx. once a month) body aches which lasted several days. These were also accompanied with chronic coughing. Unlike the flu, I typically had no fever. Some of those seemed to happen shortly after visiting family members during the winter holidays.
Saturday, Feb 20th — THE Stroke
During the week of February 15th, 2016, I was beset by another one those “body ache illnesses.” On the afternoon of the 19th I went to bed early, at around noon and slept off and on until the following morning. Rebecca and I had a memorial service to attend that day in Provo. After waking up, at about 9 a.m., Rebecca detected something was wrong. She called me by name but my response was in partial sentences. She asked me other questions, none of which I could answer correctly. Detecting a stroke, she ordered me to get dressed as she was taking me to the local Mount Pleasant E.R. I complied, after getting dressed and tying my shoes by myself (with no apparent problems).
And so began the long process of discovering about this illness, which I thought only happened to those unhealthier or older than I. This was my first-ever stroke. Both my parents suffered strokes, but at a more advanced age, so I thought I was exempt, especially I was uber fit, having done a lot of cardio activities for the past decade…and also because I “generally” ate well, while watching my weight.
Upon arrival at the Mount Pleasant Hospital they first gave me a CT scan, but because there was not time for me to drink the dye, it was non-contrast and showed no stroke. They were ready to release me, after which Dr. Day (my general physician, who was working the floor that night) arrived and suggested they keep me overnight for observation. Later he had me take a MRI and it showed definite signs of a stroke.
From there I traveled by ambulance to Utah Valley Hospital in Provo, Utah where I was admitted as a stroke patient. Eventually they gave me a brain MRI which showed that I had ischemic embolic stroke in the left frontal lobe. (This is the most common and less severe, compared to a Hemorrhagic stroke; click for more info: Visual Guide to Understranding Stroke slideshow from WebMD).
Saturday night I was unable to converse with the many visitors that came. Because of the location of this stroke I had what is usually referred to as expressive Aphasia. The outward symptom was the inability to finish answering direct questions. I could not complete my whole name or state my birthdate when asked. I could not count to 5! I really struggled with names of family members or friends. But I appeared to have little, if any physical ailments, like asymmetrical strength of my limbs or face.
Tests & results performed in Provo were (with many more in the weeks to come in Mount Pleasant and SLC):
Computed Tomography (CT) scan which showed no significant stenosis (narrowing) or occlusion (blockage?).
An EKG/Telemetry was negative for atrial fibrillation (AFib).
Heart Ultrasound (TTE) showed left Ventricular Hypertrophy (thickening of the heart wall*), right to left shunt (very small hole or PFO in my heart was discovered).
Hgb A1c: 5.5 (blood glucose, i.e. I didn’t have diabetes)
*This is OK as many endurance athletes have slightly thicker walls, i.e. 1.3cm compared to 1.1cm for the average Joe.
Results:
Initial NIHSS: 4 (stroke severity scale; patients with a number of 4 or less generally have favorable clinical outcomes). 1–4 = minor; 5–15 = moderate; 16–20 = moderately severe; 20-40 = severe. Less then 14 have an 80% change of good outcome.
Sleep apnea testGranddaughter “get well” card.Utah Valley HospitalThyroid ultrasound
Sunday, Feb 21st — 2nd Day in the Hospital
A speech therapist stopped by and gave me some “Stroke Quizzes.” Some had me naming an illustration of common items, like a feather, glove, shoe etc. I could not name a one!
Monday, Feb 22nd — Visit with the Neurologist
On Monday I was seen by Dr. Call, a neurologist from Provo. His primary job is working with stroke victims in this hospital and works at the local Stroke/TIA clinic. He was very generous with his time spent at last an hour explaining things to us. He ordered another CT scan but with dye. He suspected cancer and wanted this test for this purpose. One of the scans they saw some nodules in my Thyroid.
He also indicated that I had some heart irregularities, consequently, upon my release, upon my release, they put me on a 30-day heart-rate event monitor. This cell-phone-looking device tracks my heart rate and sends continual data via cellular phone lines to a central location for evaluation late. Additionally, this device has a manual transmitter, so if I start feeling crappy with a bad symptom, I can transmit that to the “center.”
On Saturday on Sunday I could not read English text, but on Monday, upon waking up was able to! It just happened! Wow, quick improvement. The speech therapist gave more extensive tests and could answer with an approximate 85–95% accuracy.
Tuesday, Feb 23rd — Discharged from Utah Valley Hospital
Dr. Call, the neurologist came by again visited. Some of the CT scans didn’t include enough of my lungs, so I did some more imaging. I visited with an occupational therapist who gave me more more detailed tests compared to the physical therapist on Saturday.
Prior to getting discharged I was hooked up to a 30-day heart monitor test. This is a system where three adhesive patches are attached to my chest and those wires go down to a pager-sized device on my belt. That device, then sends a wireless signal (Bluetooth?) to a modified mobile phone, which in turn sends my results to a center in Texas. Cost for rental of this device (including the lab results): $7,000! This is an excellent way of determining if one has Afib because it will show up easily on such a test. As it turns out, after 30 days of wearing this device 24/7 (except when showering), it proved I was exceptionally healthy (heart rate dropping down to an average of 33 BPM for a full minute while sleeping once) and had no apparent Afib or other heart rhythm problems.
Late in the afternoon, I was released to go home. Since it was late in day, we spent the night with family in Provo and went home the following day. The one thing that Rebecca are still searching for is the “root cause.” Some athletes have speculated that ultra-endurance activities might actually harm the heart if done in excess. Some of them suggested I have AFib and that is yet to be determined. (More Info? Living well with Artrial Fibrillation, AFib Slideshow from WebMD).
Wednesday, Feb 24th — Back in the E.R.
Just before we left Provo, I sat up from a couch and felt a little dizzy. This was something new. But sitting down I felt fine, so we left anyway as Rebecca was driving. I felt fine all the way home, in fact I was little more chatty than usual. We had a water bottle in the car and I sipped water on the way home…but not in excess.
Upon arriving home I needed to visit the bathroom and quickly made it into the house, but when standing or even sitting up I was very lightheaded. I collapsed on our bed—but I could not even sit up without feeling faint. I entered a short report into my event monitor. Then, Rebecca and I weighed our options. She couldn’t possibly get me back into the car, so she called 911. 15 minutes later an ambulance arrived and took me to our local hospital. After another CT Scan and more blood tests found nothing new (again, what’s new?). I think I was dehydrated, which brought on this lightheadedness. I was later released to go home and felt much better after getting some I.V. liquids pumped into me.
Monday, Feb 29th — Sleep Apnea Test
Per the recommendation of the neurologist, I did an overnight sleep apnea test in Provo. Some strokes are caused while one sleeps, or this test may reveal a cause of strokes. They attach numerous wire patches over your body including your feet, to determine how much you move during the night. They also monitor your heart rate to see if it does anything dramatic. I had 7.5 “events” per hour (stop breathing). Typically, they don’t even consider it a problem until one has at least 15 per hour. Also, my baseline oxygen was 99% and anything below 88% is a basis for concern. So in summary, I passed with flying colors.
Friday, Feb 26th — Prostate
Visited with my local General Physician and he put my on Flomax (prostrate, unrelated to the stroke).
Monday, Feb 29th through March 19th — Physical Therapy for Balance Problems
Appointment on the Feb. 29th with the physical therapist (P.T.), but felt very lightheaded and cancelled. Instead, I visited with my G.P. again. He suspected it might be a side affect of Floxmax (later confirmed by reading the Rx tech sheet), so he immediately pulled me off this medication. P.T. Appointment. He started me on some balance exercises, especially those for my left “bad” ankle from a 1980s ice climbing injury.
I had continued lightheadness during this time so I continued therapist sessions. He recommended balance exercises and saw small improvements during the week. I continued exercising (indoor spin bike or walking/light jogging) and increased the duration and intensity each day. Sunday, the day I didn’t do any cardio was the worse—out of balance and vertigo when I stood up etc. Is that because I did not workout? This whole situation finally cleared out, but very slowly.
Tuesday, Mar 1st — Three Different Tests
First, in Provo, I visited with a prothesis company regarding my “bad” ankle skin graft problem and how it prevents me from skiing. He provided a small foam patch to stick on the inside of my ski boot.
Second, I (we, Rebecca & I) visited with a speech therapist who wondering why I was even there. “You don’t seem to have any lingering speech affects from the stroke.”
They saw some nodules in the Provo hospital while getting imaging for the stroke and suggested get an ultrasound of my throid. Those results were forwarded to my general physician who suggested I visit with an endrocinologist.
Thursday, Mar 17th — Three Doc Appointments in One Day
One of the images of my lungs showed some nodules, so it was recommended I visit with a pulmonologist in Provo. Upon reviewing my imaging, he declared that the nodules in my lungs were “nothing,” but he wanted to see me again for some tests on my mild asthma. We discussed my asthma, which is very mild and flares up once in a great while. I also discussed with him the fact that when I get sick with a cold or sometimes the flu, I cough for weeks on end. He recommended I come back and do a breath test and then discuss the results.
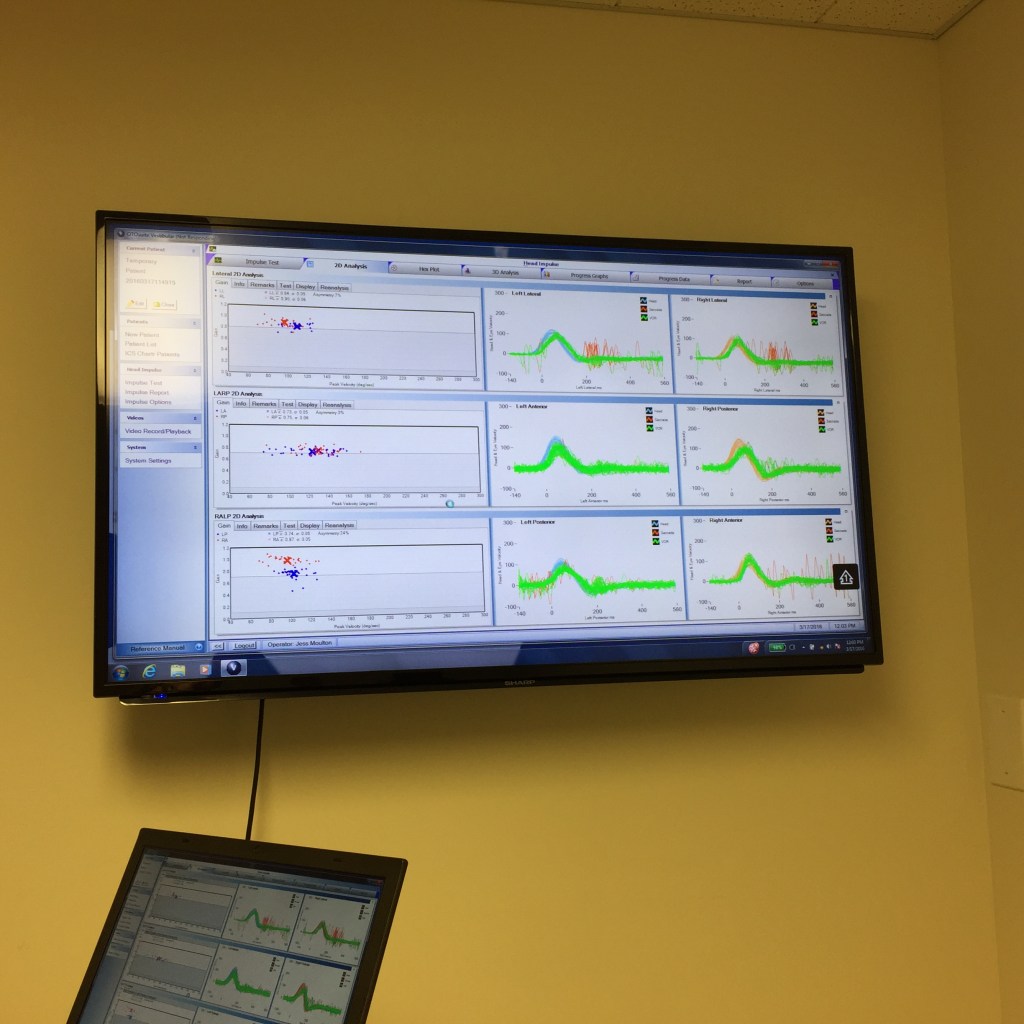
The second appointment was with a ENT (ear, nose, throat specialist who also does balance issues. The purpose of this appointment was to determine whether or not my balance problems were related to something haywire in my ears or whether it was perhaps stroke caused. Once again there was nothing wrong with my “ear-based” equilibrium.
The last appointment was with the neurologist assistant. He determined that my healing was going well, but had no answer as to why I was experiencing slight dizziness or lightheadedness. That leaves the only probable cause as the medication (Flomax) and/or a combination of low blood pressure. In any event, he said I was free to participant in normal activities, knowing that I still had appointment with a cardiologist (regarding the small hole in my hear, or PFO, which may have been the root cause of the stroke).
Tuesday, Mar 29th — Endrocinologist Visit
This was triggered by imaging of my neck and lungs — they thought they saw some nodules in my thyroid. He took a blood test (which proved all is well) and did an ultrasound and said to come back in six months to see if they have grown or changed.
Friday, April 1st — First Cardiologist Meeting
A friend of mine, who is a Doctor of Physical Therapy in Salt Lake suggested I see a certain cardiologist in Salt Lake. In her opinion, this guy was one of the two best “experts” in Utah in finding the cause of strokes. His schedule was booked up for sometime, but he kindly double-booked me so we could be looked at sooner, rather than later. I think he was perhaps intrigued why such a healthy person, with no other contributing factors, had a stroke. He looked at my 30-day heart monitor test and found nothing unusual there. He visited with Rebecca and I and recommended a patent foramen ovale (PFO) closure, which is an out-patient procedure with very low risk. My PFO was discovered in Provo, the day after the stroke through an ultrasound, so this was not a big surprise. A PFO is a small hole or gap where a curtain separating the two chambers of the heart isn’t closed all the way. 25% of all humans have this condition, something of a very minor birth defect. It is rather controversial as to whether or not it really causes strokes. What they do is take a small GoreTex type disk (about the size of a quarter) and place it over this hole, plugging it up. Later, the skin grows over it. Rebecca and I did a ton of online research, sometimes til 3:00 in the morning (coupled with much prayer and contemplation). We (or primarily “I”) decided to go for it. She had reservations, but I felt it was the appropriate thing to do.
Friday, April 14th — Discovery Day
This was a big day in the sequence of events.
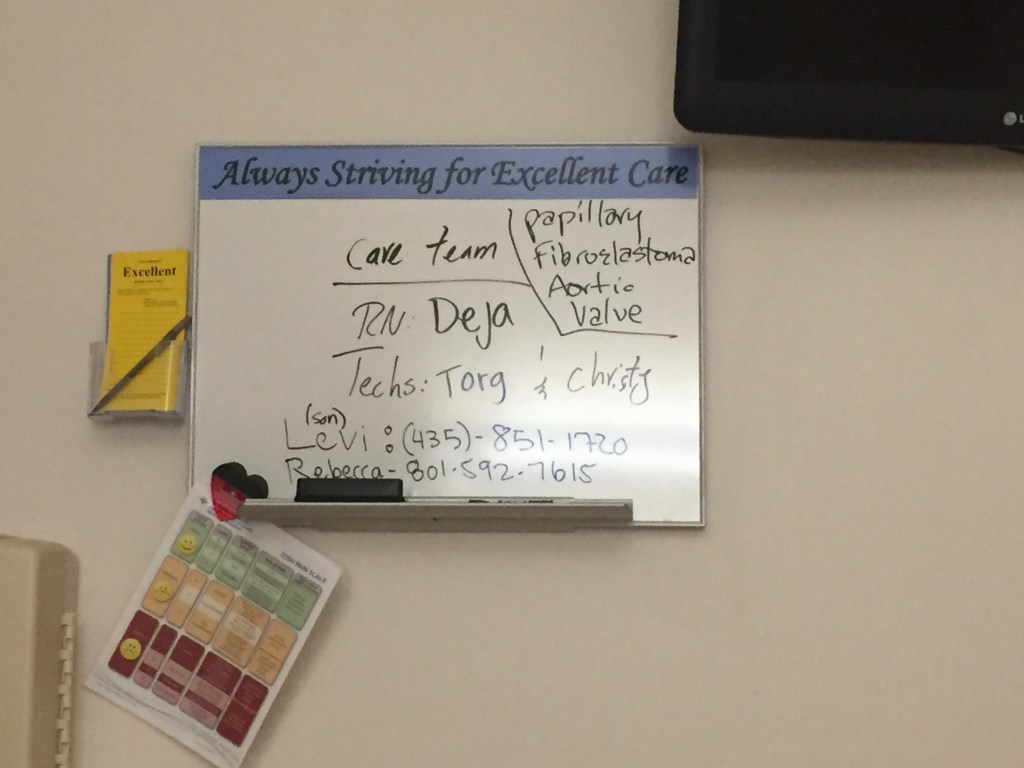
I was scheduled to get PFO closure. Prior to this procedure this cardiologist did a transesophageal echocardiogram (TEE). It is an ultrasound of the heart and reveals more detail than an MRI, X-ray or CT scan. They had me sedated and then shoved a tube down my throat which shoots an ultrasound picture from behind. As I understand it, because the ribs or other organs are not in the way, they can see more of what is happening. He immediately discovered something very odd — a growth or lesion near the left or aortic valve. It appeared to be a papillary fibroelastoma (PFE), which is a typically a benign tumor or lesion of the heart. But they weren’t 100% sure. Needless to say, cardiologist did not preform the PFO closure that day. Instead he sent in one of his cardiothoracic surgeon colleagues to talk to me about surgery to remove it — that is open heart surgery! I said, we can schedule you next week, OK? Needless to say, I was taken back and needed more time to think about my options.
Meanwhile, my cardiologist sent my images off to the acclaimed Mayo Clinic for their opinion. A week or two later they responded. They thought it might be simply a blood clot, but they really weren’t sure. He gave me two options: try blood thinners (or anticoagulants) for a month and see of this lesion disappears. The second option was to do open heart surgery to remove it. After much deliberation, Rebecca had the strong impression that it was not a simple clot and that surgery would be the best option. I concurred so I nervously scheduled a date.
Thursday, April 28th — Second Pulmonologist Appointment
I did did a pair of exhale tests, in which they had me use a rescue inhaler in between. It was obvious that I had a problem and that the Albuterol inhaler helped by a whopping 29%. He placed me in a twice-a-day maintenance steroidal inhaler, with a follow up appointment later that summer.
Monday May 9 — Pre-Surgery
I was scheduled for surgery on the 10th, but they needed to do preliminary tests the day prior. This was in building seven of the Intermountain Medical Center (IMC) in Salt Lake. This campus has many buildings, each providing services of differing specialists. The entire 7-story building I was in was for treatment of heart and lung patients. I had more blood drawn and another TEE and a Cat Scan A. The surgeon came by at about 7:00 p.m. to discuss things for the next day. He said that the surgery should be relatively simply, once they got me opened up (cutting my sternum in half). There was a very small possibility that the valve might get damaged in the process, so he asked me what type of valve I would want, if that was necessary. I indicated that a biological or pig valve would be best, compared to a mechanical valve, which requires one to be on “blood thinner” drugs forever. Later that night, at about 3 a.m. I heard a loud female voice in a nearby room. A nurse (or aid) was speaking to a patient saying “Lisa, can you hear me? (no response), Lisa, can you hear me? (no response, & this time with more fervor), “Lisa, can you hear me?” I never heard a response. Moments later I heard many people running (not walking) up and down the hall. A few minutes later I heard a male voice saying “what is going on here.” The footsteps continued and then ten or so minutes later, things got much quieter. The next morning, at about 5 a.m. I commented to the male nurse, who was in my room making the rounds, “you had a lot of drama last night, didn’t you?” I asked him what the final outcome was. He simply said “she didn’t make it.”
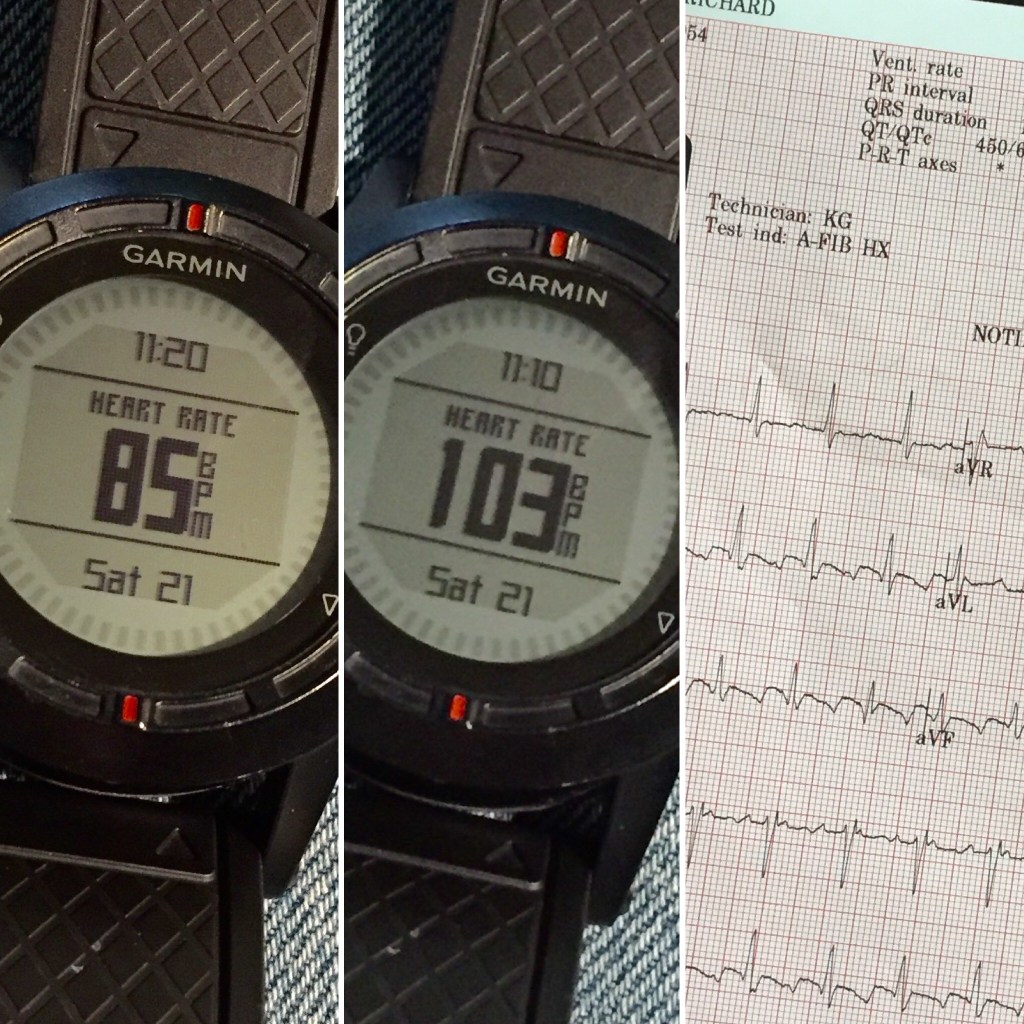
Variations of heart rate, monitored during my Afib phase with my own gear (and the EKG report shorty thereafter).EKG test showing AfbibBack in the ER (post surgery)IMC “Strip Mall” Super Hospital in Murray (SLC) Utah.Permanent zipper.FamilyWires in chest. These were used to raiser or lower my heart as needed…as easy as turning the temperature of your oven up and down!My room in IMCHoses deeply buried in my chest cavity.These chest tubes were inserted rather deeply to allow drainage. Next to them were three wires that were attached near or on my heart.Daughter Hannah and RebeccaSiblings: Susan, Sherri and Julie.Incision coveredDaughter RoseER in Mount Pleasant with Afib (note high heart rate of 95)Breath testPost surgery wires and tubes everywhereThe board that changed daily with each shift change.Surgery centerBalance test by ENT Stroke care here30-day heart monitor gearStroke chart
Tuesday, May 10th — Surgery
My surgery was schedule for late morning, or whenever the surgeon finished his prior procedure. It turned out to be much later, at about 3:00 p.m. Prior to wheeling me into the OR, I met with the anesthesiologist, who asked what I was in for. I reaffirmed I was there for removal of a lesion on aortic valve and also for a PFO closure. He also confirmed again what type of valve I wanted, if that was required.
Just prior to surgery there was a small hiccup (this all happened while I was “under”). I had a stricture or tightening of my urethra (probably related to my occasional prostrate problems of the past), which required a urologist to come in and open things up, so they could properly insert a catheter.
Finally they were able to start on the surgery by cutting my sternum in half with a saw. Shortly thereafter, they put me on a heart/lung bypass machine so they could make my heart to stop breathing and proceed with the surgery. I believe I was on this machine for about 45 minutes while the surgeon removed the lesion (cut it out) and then stitched closed my PFO. The lesion was about 30mm long (1-1/4″) and the diameter of string. It would go to a lab for analysis. They then wired shut my sternum and then put tape-like butterfly bandages to close the incision. No valve replacement was required. That was my first question I asked when coming out anesthesia, was regarding the valve, according to my daughter Hannah, who was there at that moment. I don’t recall asking that question however. I spent about 18 hours in the ICU before transferring me to a regular room. The nurse there was a real pro as she was older and very seasoned.
May 11th–14th — Hospital Recovery & Lab Results
The culprit — giant Lambl’s excrescence, 30mm (1.25″) long and the diameter of a piece of string. The O.R. nurse called it simply a “stringy thingy.” (Color is due to lab dyes).
For next four days, I recovered in a regular patient room in this building. Everyone on my floor was there for lung and/or heart problems. Naturally I was on pain meds which were moderated by how much I felt I needed them. I had many visitors which was greatly appreciated. Rebecca spent the nights with our daughter, about ten minutes away. She came and graciously spent the whole day there (while missing a week of school). Each day the physical therapists took me on two walks to keep my system moving. The anesthesia contains a drug that causes constipation, so I really didn’t have any BM’s until after I got home. I tried to drink plenty of fluids which went through my system through the catheter and into a container for measuring. I also had a Y-style hose (about 15mm in dia.) that came out of my chest cavity. This allowed my system to drain out all the gunk from the incision and surgery.
On Thursday (as I recall) my cardiologist came by with the lab results from the “thing” which was removed. Instead of it being a papillary fibroelastoma of the aortic valve (PFE) it was shown to be giant Lambl’s excrescence. Either way it was benign, and it was GONE! Rebecca, after doing research after this announcement, found that this weird lesion was almost without fail, THE probable cause of strokes, based on her online research.
It seemed like the only way I could “escape” from the hospital was if my chest drainage got below a certain amount in a six or 12-hour period of time, which it finally did on Saturday the 14th. On Friday a nurse removed the bandage covering my sternum suture and the hoses. On Saturday another nurse removed the three wires that were there to control my heart rate if needed (they needed to increase it in ICU as I got too faint; they just “dial it up or dial it down” as required).
May 15th–16th — Home from the Hospital and then my 3rd Trip to the ER
Rebecca drove me home on Saturday and that evening I developed a fever of 101F and had a fast heart rate — something I didn’t have while in the hospital. Naturally she was very concerned as the hospital was a two-hour drive. She called the 24-hour hot-line and the doc just to take some Tylenol and call him in the morning! I took the meds and immediately went to sleep, on my side! In the hospital, with all the hoses and wires attached, I couldn’t rotate onto my side. That night I did and it was wonderful, yet for the next six weeks I ended only being able to sleep on my back due to sternum pain.
On Sunday the 16th my fever dropped a little, but my heart rate was escalated and was erratic. Finally, late in the day, I had enough sense to wear my Garmin with a chest strap to determine what my heart rate was. It was reading 130-140 resting! This couldn’t be right, so we (Rebecca) called the hot-line again and he said to go to our local hospital and get an EKG, which we did at about 10:00 p.m. It revealed I was in atrial fibrillation (Afib). The ER doc said it was not usually fatal and just chill for the night. It seems like by 2:00 a.m. they gave me some meds to slow my heart rate down, but it did nothing. At that hour, instead of going to a regular room in the hospital I just attempted to sleep on the rock hard gurney all night, while Rebecca went back home to rest and get away from watching the heart rate machine above my head. The next morning my local general physician, who had been notified, stopped by. He called my cardiologist, who said to make the trip back up to Salt Lake for a procedure.
Before leaving my local Mount Pleasant hospital they gave me a shot in my stomach with a heavy-duty anticoagulant (blood thinner). Immediately, upon walking out of the hospital I felt weakness in my left leg. Later on, my back ached causing me to hunch over for the better part of a week. This was due to sleeping on the lousy gurney all night or as a side-affect of this new medication.
In Salt Lake they first sedated me with an I.V. and gave me a TEE to see if there was any blood that had pooled in my heart, which would cause another stroke. There was none evident, so they proceeded with a cardioversion, which is essentially shocking the heart with paddles. It brought my erratic heart rate down, so they sent me home. Well actually, I didn’t go home as I had an appointment with a urologist the next morning, so I stayed at my daughters home and then later went home on Tuesday the 17th.
May 17th–25th — Afib Resurfaces
For the next week or so, I just slept a lot (on my back) and did some light office work like checking email. Per the surgeons order, I started walking twice a day, starting with 5 minute walks (which seemed like nothing as I had more energy than that!) and increased the time each time, building up to 60+ minute “power walks.” I also did some indoor spinning (w/o holding onto the handlebars) for some of those days too. My heart rate seemed to be doing OK. I kept it under 130 BPM as per docs recommendation. My sternum didn’t hurt a ton and I didn’t seem to have much pain. I was off pain meds before the left the hospital. On Monday the 23rd, my Atfib returned, but not as bad as before. And so on Wednesday the 25th I went back up to Salt Lake and got another cardioversion (i.e. heart zapped). And once again, my heart settled down. The cardiologist mentioned that this is frequent (about 1/3 of patients) after heart surgery, but it most commonly happens in the four to five days while in the hospital. Mine condition was delayed for some reason. After this second cardioversion, my heart finally settled down and Atfib never returned.
May 25th–June 15th — Sternum Pain
I was told by a friend that for the first two weeks following open heart surgery, my sternum will hurt a lot, and things will get better after that. Mine was the opposite. For the 10 to 14 days following surgery it felt OK (except when used an allen wrench once and torquing something…which required opioids) and then it really started to hurt. It was a constant gnawing discomfort, requiring Tylenol from time to time to get to sleep. On the 15th I visited with the cardiothoraic surgeon and since I was complaining about sternum pain he suggested I quit using the indoor spin bike, which I did for the next two weeks.
June 21st — Allowed to Drive
The following week, after visiting with the surgeon, which was some six weeks after surgery, I was allowed to drive, which is typically waiting period for all open heart surgery patients. This gave me more freedom, especially so I could drive to go on “workout” hikes in the nearby foothills, instead of just walking on pavement. They also said I could lift up to approx. 20 lbs. now.
July 1st — Cardiologist Post-Surgery Appointment
Some two weeks after visiting with the surgeon, the cardiologist wanted to check on me. At that meeting, he suggested I continue using my two medications: an anticoagulant (Eliquis) and a heart rhythm pills (Amiodarone) until 90 days after my last cardioversion — so until August 23rd. I was placed on these after my first Afib episode. Had I not had Afib I would most likely had to use them at all. He also informed me that the integrity of my veins, artery and heart was in excellent shape and that unless my LDL (bad cholesterol) gets over 130 (it has been around 100), that I should never need to be on any long-term meds (other than a daily inhaler), especially since I am so active, have a decent body weight, have a low resting heart rate and have normal (if not low) blood pressure. He also said the surgeon was full of it and I could resume indoor spinning, as long as I was not holding onto the handlebars and standing up to pedal, so as to damage my sternum.
I did ask what caused this lesion of the heart and he said the medical community had no answers as to the root cause — a total random occurrence. He did not say that ultra-endurance activities would contribute to it.
July 6th — A Sudden Improvement in Sternum Discomfort
At 7-1/2 weeks post surgery my sternum suddenly become less of an annoyance, especially at night while trying to get to sleep. I had been sleeping mostly on my back with extra pillows including a big triangle pillow to simulate a hospital bed. The discomfort of the sternum had a cyclical throb, especially at night. In early July it finally subsided just enough so I could sleep on my side without pain. What a relief. It seems to have continued to improve with additional week of healing.
The Future
As of July 2016, the cardiologist recommended that I not cycle outdoors until I am off the meds (late August, some 3-1/2 months after surgery). He did say I could now push heart rate up to it’s maximum with no worries at all — it is in excellent shape. Needless to say, I have tried to do this by hiking and doing some light “jogging” on steep trails nearby. He prefers I not run too much (plenty of hiking is OK) yet as it may hurt the sternum. In the past, I have had issues with running, due to old mountain injury which now causes me much pain in the joint of my left ankle. I have been told it is basically “bone on bone.” So I began investigating different ankle braces and discovered a new one and also purchased some very cushy trail running shoes (Altra Olympus 1.5…the new 2.0 has a much better sole for loose trails). This has given me a new lease on my endurance training, as I can now go for a three or four hour “power hike” with little or no pain. My next event is a family trip up Mount Rainer in mid August, so I am doing a lot hiking and some jogging in an effort to get in shape for this 10,000-foot climb.
Less important, but a possible positive byproduct of this year’s health unrest, is the fact that my VO2 Max (ability to use oxygen while exercising), may be increased through the regular use of a maintenance inhaler, as advised by my pulmonologist. It is most likely though, that this medication will increase my VO2 Max. Whether or not this increases, it is my understanding that this will improve or reduce these bouts of chronic cough. My cardiologist, on the other hand, does not seem to think that removal of this lesion will improve myVO2 Max, but perhaps, this heart condition was a contributing cause to my frequent coughing “body ache” sessions.
In late August, I plan to get back on a real bike, outdoors, and restart my road cycling training regimen…perhaps mixed in with more running (i.e. cross training), especially in the early winter, when it is uncomfortable to cycle, yet too early to backcountry ski.
Lessons Learned
Since about 2007, I have been doing ultra-endurance sports: running (ultra means more than 26.2 miles…sometimes up to a 100 miles straight without sleep or a long break) and road cycling (ultracycling or randonneuring…sometimes up to 500+ miles without significant stops). With cycling, becoming more fit means that: a) many times, I could hang with guys much younger, taking advantage of drafting, a significant time and energy saver and b) I could get more sleep on timed multi-day events like a 1200km (750-mile) brevet. Consequently, I have tried to remain as fit as possible (including mentally “fitness”), but to the chagrin of my family, who, as a general rule, do not enjoy or support endurance sports much.
Many of us humans, through major medical situations (including childbirth) or crises, are compelled to be humble, or our relationships with our loved ones (and friends) become more strengthened. I believe that is case with my Rebecca, as I cannot tell you how important it was for her to accompany me to the various doctor appointments, to help “interpret” or “spiritually sense” what was best as we received medical guidance or sometimes advice that was conflicted. She sacrificed a bunch of time and missed one of her all-time favorite things in life: teaching, in order to be there for me.
Preparedness. Are we mentally and spiritually prepared for unforeseen drama in our lives? Are we financially prepared for such situations? Is our insurance able to cover for such surprises (I believe the total for this year will be about $100,000). Having a spouse with a stable personality and a raw intelligence and spiritual toughness has been a true blessing of preparedness, I believe. Because of her teaching job, we have assume insurance, which has helped reduced the stress in an already stressful situation.
In late 2015 I had planned on doing two 1200km brevets (3-5 day 750-mile bike rides) in 2016—something I had not done in one season and wanted to do before I become too aged (I’m 62). And then, my plan was that in 2017 to reduce my overall volume of training and long rides. But…the powers of heaven had something else in mind for me. Sometimes our timeframe is the not His or His way is higher (or different) than ours!
As mentioned above, not be able to cycle for a period has forced me to find other ways of staying fit (through the discovery of a new style of ankle brace & better running shoes), i.e. “speed hiking” or simply walking as fast as possible up steep trails for fitness. Although I will never be able to do any ultra-length runs, I have a renewed interest and ability in walking or light running as an alternative to cycling and randonnée or backcountry skiing.
I suspect in the coming months I will discover other divine purposes for all this and may (or not) publish them here.
If you any comments or thoughts, please post them here so-as to share with others, rather than e-mailing me directly.
atrial septal defect (ASD, similar to a PFO, but smaller)
cardiac catheterization. Coronary angiography is done during cardiac catheterization. A contrast dye visible in X-rays is injected through the catheter. X-ray images show the dye as it flows through the heart arteries. This shows where arteries are blocked.
cardioversion. Rezapping of the heart with paddles in a controlled environment in a hospital, but unlike that which is administered to an unconscious person (i.e. by an EMT), the patient is sedated so as it not remember the whole procedure. Used to stop arrhythmia or Afib.
giant Lambl’s Excrescence (on of the aortic valve, typically a benign tumor or lesion
patent foramen ovale (PFO or small hole or opening between the curtains between the heart chambers)
papillary fibroelastoma (of the aortic valve, PFE, typically a benign tumor or lesion)
systemic embolism (S = transportation of oxygen to the body in general, as opposed to the lungs. E = blood clot or gas bubble in bloodstream)
transesophageal echocardiogram (TEE, or an ultrasounds of sorts of the heart)
transthoracic echocardiography (TTE, similar to an TEE, but different?)
Strokes, PFO & Other Research Links
Prior to getting my PFO closure, Rebecca and I spent many a late night researching this. The research seemed to indicate that it had very marginal benefits. I did ask my cardiologist about this and he said that the most recent complete study, the RESPECT study (link below), was somewhat flawed as some of the patients that had no problems, exited the study early, thus leaving the “bad apples” to mess up the average.
Blue Cross of Idaho summarizes three different studies indicating none where effective. FPO Transcatheter is investigative; Transcatheter of ASA is Ok as it is FDA approved. For ASD, it is OK; for stroke ??? CLOSURE I, RESPECT and PC studies included. https://www.bcidaho.com/providers/medical_policies/med/mp_20209.asp
American College of Cardiology: The results of the RESPECT trial indicate that PFO closure with the Amplatzer PFO Occluder is not superior to medical management in reducing recurrent strokes in patients with presumed cryptogenic stroke and evidence of a PFO. There were, however, trends toward benefit on per-protocol analysis and in patients with large shunts and those with atrial septal aneuryms. On extended follow-up, the results were mostly similar. An interesting observation was that nearly one third of strokes thought to be cryptogenic likely had another underlying mechanism, and in patients with true cryptogenic strokes, PFO closure appeared to be superior compared with medical management. http://www.acc.org/latest-in-cardiology/clinical-trials/2013/07/19/12/28/respect
23 page Government report with little consensus;except that the larger study may have concluded a slightly better outcome. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1768084/
Report that indicates there is no benefit but some risk with atfib. 2012. Require 2nd episode before closure unless ASA is present. http://www.medscape.com/viewarticle/820831
“ASA is not a true aneurysm, but is best defined as a “floppy” septum that bulges into the right and left atria during cardiac cycles…Should we close the PFO? We believe that in spite of the absence of a multicenter-controlled study, there is a strong case for the closure of a PFO in a young patient following a cryptogenic stroke or TIA. The strongest case exists in patients with a co-existing ASA.” http://www.cathlabdigest.com/articles/The-Rationale-PFO-Closure-A-Series-Arguments-For-or-Against
2012 report by the Mayo Clinic entitled: Potential Adverse Cardiovascular Effects From Excessive Endurance Exercise. The conclusion says: Consensus Guidelines for Physical Activity and Public Health from the American Heart Association and American College of Sports Medicine call for at least 150 minutes per week of moderate ET or 75 minutes per week of vigorous ET in the general adult population.1 Those guidelines also suggest that larger doses of ET may be necessary in some groups, such as those with or at risk for CHD (30 to 60 minutes daily), adults trying to prevent the transition to overweight or obesity (45 to 60 minutes per day), and formerly obese individuals trying to prevent weight regain (60 to 90 minutes per day). The guidelines also caution that high-intensity ET increases risk of musculoskeletal injuries and adverse CV events.1,42
Most GPS units or heart rate monitor watches ask for your maximum heart rate so it can calculate the different heart rate zones. I have outlined several different methods below. Please note that your maximum heart rate is different than lactate threshold. As per this article in Road Bike Ride, by John Hughes, “Max heart rate doesn’t show cycling fitness,” but instead “lactate threshold is a better measure of fitness.” I have covered that topic on this blog post.
Here are some formulas for determining your maximum heart rate:
The old classic easy-to-use formula is 220 minus your age for males or 226 for females. But is a very rough estimate and can vary widely.
Here is another formula, perhaps more accurate than the above: “The maximum heart rate of male athletes was calculated to be 202 – (0.55 x age), and for female athletes, 216 – (1.09 x age).” From the RBR site and is Dr. Mirkin’s formula from a study in Liverpool England.
I believe this is most accurate technique, by Edmund R. Burke, PhD, as found on pg. 74 in the timeless book Serious Cycling (2nd Ed).
Do an all-out effort on a 5 km (3 mile) time trial (solo and a generally a flat course). Determine your average heart rate in the middle of this ride. He says. This is your exercising heart rate. Manually plot your heart rate against your time and speed on a graph. You’ll see that your heart rate levels off in the midportion of the ride. This corresponding heart rate is your average heart rate. Multiply that number by 105 percent to arrive at your maximum heart rate.”
Sally Edwards, in her book The Heart Rate Monitor Book, suggests…
finding a long hill or series of hills and, after warming up, hitting the bottom of the hill relatively fast. Work the hill extermely hard until your heart rate reading no longer rises and you approach exhaustion. This number is your maximum heart rate. (Quoted in the book Serious Cycling above.)
It would seem to me that if you race (as opposed to just training or causal “riding” with friends), that taking your highest recorded heart rate during an event would yield the same result as Sally’s method above.
Have a medical professional conduct a stress test and let them know you want to know your absolute maximum heart rate. This is usually done on a treadmill, however, and not on a bicycle, which may yield a slightly higher value.
Sigma of Germany makes some nice heart rate monitor watches and cycling computers. Here is their formula, from their PC15 instruction manual (circa 2007).
First, convert your weight from pounds to kg: divide by 2.2. Then for men: 210 – “half age” – (0.11 x weight in kg) + 4 Or for women: 210 – “half age” – (0.11 x weight in kg)
Also visit this page on my blog about anaerobic or lactate threshold.
In addition to my twice-a-week strength training regimen I now carry a hand strengthening device in my car. I use it when traveling or running errands. I originally started using a regular “hardware store” scissor clamp (background — yellow clamp), but it failed after about two months of use. I then picked up this clamp from Flawless Fitness on Amazon. I have used it for a few months now and it seems to work great. It is adjustable in the pressure and opening.
Why bother? Read on.
For doing pull-ups, it aids in keeping my old (60+ yr old) hands stronger for that purpose.
Having stronger hands certainly helps when changing out tires and/or tubes.
In 2012, while on a the Colorado High Country 1200K ride, I was able to work with a small group of fellow riders for this 4-day event (translation: they were kind enough to let me draft with them!). For some reason, towards the end of this ride, my hand got very fatigued, to the point that after the ride, I was barely able to open my car door with my keys. I am guessing that this was due to all the gentle braking with my fingers as I was drafting for hours and hours each day. At that time I was not doing hand strengthening exercises. I am not hoping for a repeat, so consequently I have added this easy one to my “regular work outs.”
Seven takeaways from this recently (2015) released title Fast After 50 — How to Race Strong for the Rest of Your Life. By Joel Friel, author of other best-selling books like The Cyclist’s (or Triathlete’s) Training Bible, The Paleo Diet for Athletes etc. Incidentally, he just turned 70.
I didn’t start a consistent exercise regiment, until I started running when I was in my 50s. I am now 61, so this material is SO applicable for me. I never knew what it was to “race young” as I never did any competitive sports in high school or college. Even if you don’t race, it is nice to be able to have some extra speed or strength for those tough conditions like high winds while road cycling or uphill skiing in deep powder.
“Much of what science ‘knows’ about the indicators of aging probably doesn’t apply to you. You are much less likely than your ‘normal’ neighbor to contract the lifestyle diseases of aging. You aren’t normal – and that’s good. You are continuing the active and vigorous life however ancestors. You’re an athlete.” p. 21
Training volume and intensity are both important, but intensity is the most relevant factor in maintaining a decent VO2max for older athletes. p. 35. Ned Overland, in this book, says “I’ve learned that by reducing volume, I’m more rested for high-intensity sessions, and by being rested, I can push myself harder during the intervals.” p. 114
“So far, about all science knows about exercise and aging is that there seems to be an inverse relationship between older people’s volume of exercise and the risk of premature death, regardless of the cause. In other words, the more you exercise the less likely you are to die early.” p. 43 “most people ‘rust out’ due to inactivity, rather than ‘wear out’ from being overly active.” p. 45
“The older athlete, therefore, needs more protein to ensure that there is enough to help with the rebuilding that takes place during sleep.” p. 221. He says that protein is required after any strength workout or session that stresses your muscles “such as aerobic-capacity or lactate-threshold intervals, you eat some protein within 30 minutes…” He goes on to suggest that older athletes need 40 grams after such a workout, instead of the typical 20 to 25 grams of protein that is recommended for younger athletes. p. 222
I have read in many other publications and online that the best way to burn fat is to workout at a moderate intensity, and not go “all out,” working out at or near your lactate threshold. But that has always seemed illogical to me, consequently, nearly every workout I do as at a high intensity. Joel confirms my theory and he says that very low heart rate training to burn fat is a myth that just doesn’t go away. “Low-intensity, fast-paced exercise does not burn more calories or more fat than does high-intensity, fast-paced exercise.”
He recommends year round resistance and core strength training (i.e. weight lifting). Once or twice a week is usually adequate, once you establish a base. p. 122–124 & 170-173. Strength training is also widely known to prevent or delay osteoporosis. Because of the compression of joints and spinal disks, by the age of 80, most “normal, non-athletic” people lose two inches in height. p. 19
He also mentions that if a “senior” athlete is injured or takes time away from regular training and losses his or her fitness level, it takes much longer to “get back” to where you were. Younger athletes, on the other hand, can take time off and more quickly rebound without the same quantity of days and weeks of training.
Several years ago, while riding a 600K on a highway in Arizona (near the Grand Canyon), some experienced randonneurs expressed the opinion that riding at night on a highway is actually safer than during the day. Since that event, I have often wondered about this.
A few weeks ago, I did a 200K (125-mile) training ride. Because of predicted gusty winds of 40 MPH I decided to do a pre-dawn start so those winds would be to my back when they finally hit, later in the day. (This turned out to be a perfect plan as I had them to my back for the last half of these ride and was able to fly along at 27 MPH on the flats, solo…but that is another story!) Early in the ride, my route took me on a short section (~ 8 miles) of I-15, where the speed limit is 80 MPH. I had on my usual reflective clothing, which was a reflective vest and ankle bands. I also had on two red 1/2-watt blinkies, both of which were in blink mode. One on my left seat stay and the other on my ankle that goes up and down while pedaling, providing even more attention. During that section, while on the broad shoulder of the freeway, virtually every vehicle (including many semi-trucks) changed lanes to avoid me. I have ridden this same section during the day, and vehicles rarely changed lanes when they came upon me.
Later that morning, while it was still dark, and on a different two-lane undivided rural highway, which had a very small shoulder…every vehicle either swung wide as they saw my lights in the distance. Then, an hour or two later, shortly after dawn, when my lights were not bright enough to penetrate the darkness (I still had my blinkies turned on…just to be sure), vehicles were cutting me much closer. Occasionally I would ride on the outside or right side of the rumble strip when there was room, but that was not always possible. This simple test proved that on rural roads or highways, night riding was indeed safer than riding during the day.
Please note that I had my rear blinky lights blinking and not on solid mode…that tells motorists that there is either a slow-moving vehicle, person receiving a citation or an accident ahead and to slow down and/or change lanes. I completely disagree with some that state that cyclists should ride with a solid red rear light, as a blinking light causes impaired drivers to steer toward you.
Now, for riding in urban areas, night riding may be less safe as there are so many other distractions and lights, including street and store signs and the glare of other motorists headlights blinding both cyclists and motorists alike. This can be especially hazardous during the hours of dawn or dusk as bicycle lights may not be bright enough to cut through the semi-dark conditions.
Also, be aware that riding at dawn or sunset (especially while going climbing or descending in a canyon), conditions where the sun may be blinding motorists easily, it behooves you to keep your tail light on…just to be safe.
During the middle of July (2015), while riding a 600K (375 miles in just under two days…or sometimes in one long day), I reflected upon the various reasons why many cyclists fail to finish long rides. The three most common problems are listed first.
Aside from my eight points below, check out this interesting 2019 article entitled “Bad Day Syndrome,” from the CTS site.
Gastrointestinal Distress: Some endurance athletes have GI problems that cause their stomach to stop accepting food or fluids. Fortunately, I have had good luck in this area. This podcast with Ben Greenfield interviewing Allen Lin (Scratch Labs) and his theory indicates that we should be eating more solids, rather than a liquid diet. Solids will slow down your stomach emptying, thus making it more stable. This flies in the face of Hammer Products, who believe the opposite is true.
Either way, consuming electrolytes, and not just plain water is imperative to stave off bonking. How much to take is subject to discussion. I personally use the elete-brand liquid add-ins to my plain water bottle and then a sports drink to my other bottle. I use Endurox, which has protein which is good for events exceeding three or four hours, or Heed, which only has carbs, and is my favorite “subtle” flavored drink. Per Seattle randonneur David Roberts: Tums are useful for stopping cramps. Chew one at the first muscle twinge. If it keeps on coming on, chew another. Brand name Tums, regular strength work best. Again, they seem to work too fast for the stuff, whatever it may be, to get into the bloodstream, although sublingual might be really quick. It’s definitely not the calcium. Blood sugar levels are also important: When you’re trying to change a flat alone in the dark and it’s raining, maybe suddenly you find yourself crying. Eat something. Any time the idea of quitting enters your head, eat something. If your power is dropping on a long climb, eat something. Many times negative feelings can be banished by eating. The rest of the time it’s dehydration. (June 2016)
• I recently heard (May 2017) that consuming fatty foods helps prevent GI distress & sea sickness. Summer sausage & cheese are two of my favorites on climbing or backcountry skiing trips. It coats the walls of your stomach making it less sensitive to distress. • Also, check out this 2015 article on the Bicycling Magazine website.
• “This has led to the realisation that gut problems in athletes are not one-size-fits-all, and culminated in a new term, “Exercise-induced Gastrointestinal Syndrome”, which describes the numerous ways athletes can experience gut problems.” Quote from this Cycling Tips article.
• Wikipedia says that Exercise-induced nausea may be caused by “Exercising at a heavy rate causes blood flow to be taken away from the stomach, causing nausea.”
Dehydration, Electrolyte Depletion or Cramping (very much related to #1 above):
• Here is a informative article on the Ultracycling site about muscle cramps.
• An article from The Science of Sport website.
• I have heard good things about the HOTSHOT drink to eliminate leg cramping (2026).
Pressure Points: Cycling has several pressure points where you body meets the bike — feet, hands and butt. Creating a comfortable ride, sometimes at the expense of a little extra weight is worth it. For me, my downfall has always been saddle discomfort. I have had saddle sore issues since day one. Sometimes, I can go for two seasons without any problems, but then, sometimes out of the blue, things blow up. Frequently, in the spring, I test new saddles, for inclusion on my website, or as I am always seeking the “the one.” Because of that, during the process of changing out from one saddle to another, or from one bike to another, my body doesn’t get a chance to adjust long enough. Elsewhere on the blog, you will find my experiences with many different kinds of saddles.
Attitude: I came into cycling, after having done many mountaineering and backpacking trips, in both summer and winter. Those adventures taught me two things..plan and prepare well, but keep a positive attitude, as some things are just out of your control. Just deal with it and don’t quit. If the weather goes south, or you are lost, or you are experiencing mechanical problems, try to stick it out. I guess you could call me a summit-bagger. In mountaineering, we wanted to complete the climb by going all the way to top — quitting early was a DNF, something I didn’t like.
Body Weight: Many serious amateur and pro cyclists have a body weight between two and 2.5 pounds per inch of body height. It’s important to have your power and strength ratio to a point where you can climb up hills at a reasonable speed and/or go up and over rollers without too much hesitation. For me, my shortcoming is my love of wheat or gluten products, especially pastries. I also like other products foods that are high on the high glycemic index which include corn, corn chips, and potatoes. I am not saying you should be gluten-free by any means, but replacing many of the wheat products with vegetables will help a lot.
Another note on body weight during an event: if your body weight is way down during an event, then most likely you are not hydrated. On my first 100-mile ultrarun, they weighed all participants at the beginning and then later, at about the 70-mile mark. If my weight had been too low, they would have pulled me and got me on fluids until my weight was back up.
Moving Speed: Some cyclists just train alone (like me, since I live in a rural community with few other roadies), but it is very difficult to gain speed by riding alone. Riding with a small group of friends, especially those that are faster and you, will help immensely. Some folks believe that for endurance long-distance cycle if you do not need to develop speed work. I completely disagree. By doing speed work with these so-called club brides, it brings your heart rate up to a high point which is invaluable in longer rides. I also do interval work on gradual hills, but nothing matches the competitive spirit of trying to stay up with someone else while sprinting on a flat, or climbing.
Sleep: Many of us are so nervous the night before an event, that we sleep poorly, so the key is to get a solid nights sleep, two nights before big events. When doing multi-day brevets (i.e. 600 km or longer), the key is to leave each morning before the control (or checkpoint) closes. Leaving after the closing time means you are chasing the clock in a big way. When I ride 1000 or 1200K events, I need 3-5 hours of sleep each night, otherwise I just get too dang tired during the hot afternoons. Because of this, one my driving forces during my many workouts is to increase my speed, so I can get enough sleep during multi-day events.
Breaks: Recently, a good cycling friend, Kerin Huber, from California, mentioned (while we were doing a 1000K), that the key to getting a good time on long rides, it not necessarily your moving speed, but how often and how long you take at each stop. During brevets, some cyclists dilly-dally at the c-stores and eat up too much time. Others like to take multiple opportunities during the day to eat at sit-down restaurants, instead of doing “grab and go” food. I tend to like to only eat major meals only once or twice per day, while the balance of my calories is on the run, or eaten curbside.
Efficiency While Riding: Some randonneurs feel that drafting is only for racers and not appropriate while riding brevets. I believe that one should do whatever is necessary to increase your moving speed, so that if there is an unexpected problem (mechanical, GI, weather etc.) you have more time in the bank — it serves like an insurance policy. Drafting at night is OK, IF one leaves a little more space that usual. I recall on early on day one of a 1200K, that two individuals, both out outside the US, touched wheels at night and both went down, causing one to get a broken hip.
Sometimes, while riding late at night, If I am tired, having someone next to me and talking will keep me going without fatigue. Though not as efficient as drafting, it will allow one to keep on moving.